The high failure rate of drug trials
The high failure rate of drugs in clinical trials, especially in the later stages of development, is a significant contributor to the costs and time associated with bringing new molecular entities to market. These costs, estimated to be in excess of $1.5 billion when capitalized over the ten to fifteen years required to develop a new chemical entity, are one of the principal drivers responsible for the ongoing retrenchment of the pharmaceutical industry. Therapeutic areas such as psychiatry, now deemed very high risk, have been widely downsized, if not abandoned entirely, by the pharmaceutical industry. The extent to which patient noncompliance has marred clinical research has in some cases been underestimated, and one step to improving the design of clinical trials may lie in better attempts to analyze patient compliance during drug testing and clinical development. Phil Skolnick, Opiant Pharmaceuticals The Secrets of a successful clinical trial, compliance, compliance, compliance.
Compliance, compliance, compliance
Compliance is considered to be key to success of a medical treatment plan. (1, 2, 3)
It is the “billion dollar question” in the pharma and medical device industry.
In home-use medical devices in particular and in chronic diseases in general – there is wide consensus that patient compliance is critical to the success of the clinical trial. Our experience with Israeli innovative medical device vendors is that they understand the criticality of patient compliance. They “get it”.
However, as Skolnick et al note – patient compliance with the clinical protocol is often underestimated in drug trials.
There are 4 challenges for assuring patient compliance in medical device trials.
1. The first challenge is maintaining transparency. An executive at IQVIA noted (in a personal conversation with me) that IQVIA does not calculate patient compliance metrics since they assume that patient compliance is the responsibility of the sites. The sponsor relies on the CRO who does not collect the metrics who relies on the sites who do not share their data.
2. The second challenge is having common standard metrics of compliance. Site performance on patient compliance may vary but if sites do not share common metrics on their patients’ compliance, the CRO and the sponsor cannot measure the most critical success factor of the study.
3. The third challenge is timely data. In the traditional clinical trial process, low-level data queries are resolved in the EDC but higher-level deviations often wait until study-closeout. The ability of a study team to properly resolve thousands of patient compliance issues months (or even years) after the patient participated is limited to say the least
4. The final and fourth challenge is what happens after the clinical trial. How do we take lessons learned from a controlled clinical trial and bring those lessons into evidence-based practice?
A general approach to measuring and sharing patient compliance metrics
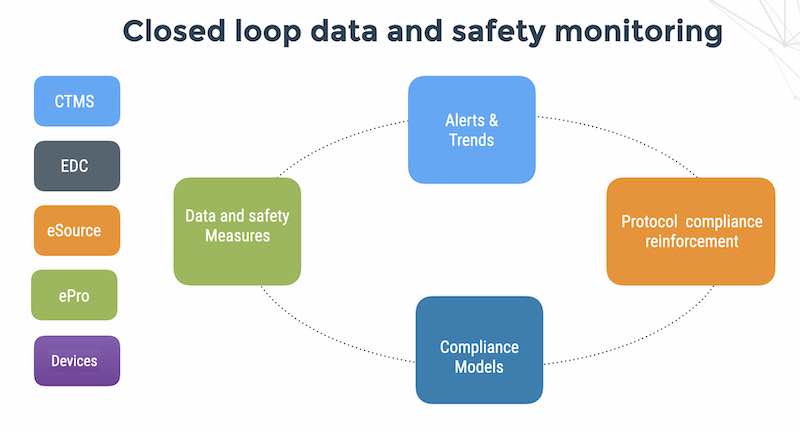
A general approach to addressing these challenges should be based on standard metrics, fast data and active monitoring and reinforcement and reuse.
1. Use standard metrics for treatment and patient reporting compliance. The metrics then become a transparent indicator of performance and a tool for improvement.
A simple metric of compliance might be a score based on patient reporting, treatment compliance and treatment violations. We may consider a threshold for each individual metric – for example a 3 strike rule like in baseball.
A more sophisticated measure of compliance might be similar to beta in capital market theory where you measure the ‘volatility’ of individual patient compliance compared to the study as a whole. (Beta is used in the capital asset pricing model, which calculates the expected return of an asset based on its beta and expected market returns or expected study returns in our case).
2. Fast data means automating for digital data collection from patients, connected medical devices and sites eliminating paper source and SDV for the core data related to treatment and safety endpoints.
3. Actively monitor and help patients sustain a desired state of compliance to the treatment protocol, both pharmacologic and non-pharmacologic. Not everything is about pill-counting. This can be done AI-based reminders using techniques of contextual bandits and decision trees.
4. Reuse clinical trial data and extract high quality training information that can be used for evidence-based practice.
Patient compliance teardown
Measures of patient compliance can be classified into 3 broad categories:
Patient reporting – i.e how well patient reports her own outcomes
1. Treatment compliance – how well the treatment conforms to the protocol in terms of dosing quantities and times of application. 2. Research suggests that professional patients may break the pill counting model
3. Patient violations – if the patient does something contrary to the protocol like taking a rescue medication before the migraine treatment
Confounding variables
Many heart failure patients are thought to be non-compliant with their treatment because of prior beliefs – believing that the study treatment would not help them. In the European COMET trial with over 3000 patients it was found that a Lack of belief in medication at the start of the study was a strong predictor of withdrawal from the trial (64% versus 6.8%; p < 0.0001). Those patients with very poor well-being and limited functional ability (classified as NYHA III–IV) at baseline significantly (p = 0.01) increased their belief in the regular cardiac medication but not in their study medication (4)
But numerous additional factors also contribute to patient non-compliance in clinical trials: lack of home support, cognitive decline, adverse events, depression, poor attention span, multiple concomitant medications, difficulty swallowing large pills, difficult-to-use UI in medical devices and digital therapeutics and inconveniences of urinary frequency with diuretics for heart failure patients (for example).
It seems that we can identify 6 main confounding variables that influence compliance:
1. Patient beliefs – medication is useless, or this specific medication cannot help or this particular chronic condition is un-curable
2. Concerns about side effects – this holds for investigators and for patients and may account for levels of PI non-compliance.
3. Alert fatigue – patients can be overwhelmed by too many reminder message
4. Forgetfulness – old people or young persons. Shift workers.
5. Language – the treatment instructions are in English but the patient only speaks Arabic.
6. Home support – patient lives alone or travels frequently or does not have strong support from a partner or parent for their chronic condition.
Summary
Flaskdata.io provides a HIPAA and GDPR-compliant cloud platform that unifies EDC, ePRO, eSource and connected medical devices with automated patient compliance monitoring. The latest version of Flaskdata.io provides standard compliance metrics of patient reporting and active messaging reminders to help keep patients on track. Your users can subscribe to real-time alerts and you can share metrics with the entire team.
Contact Batya for a free demo and consult and learn how fast data, metrics and active reinforcement can help you save time and money on your next study.
References
1. Geriatr Nurs. 2010 Jul-Aug;31(4):290-8. Medication compliance is a partnership, medication compliance is not.
Gould E1, Mitty E. https://www.ncbi.nlm.nih.gov/pubmed/20682408
2. Depression Is a Risk Factor for Noncompliance With Medical Treatment: Meta-analysis of the Effects of Anxiety and Depression on Patient compliance. DiMatteo et al http://jamanetwork.com/journals/jamainternalmedicine/fullarticle/485411
3. Importance of medication compliance in cardiovascular disease and the value of once-daily treatment regimens. Frishman. https://www.ncbi.nlm.nih.gov/pubmed/17700384
4. Adherence and perception of medication in patients with chronic heart failure during a five-year randomised trial Ekman, Andersson et al. https://doi.org/10.1016/j.pec.2005.04.005